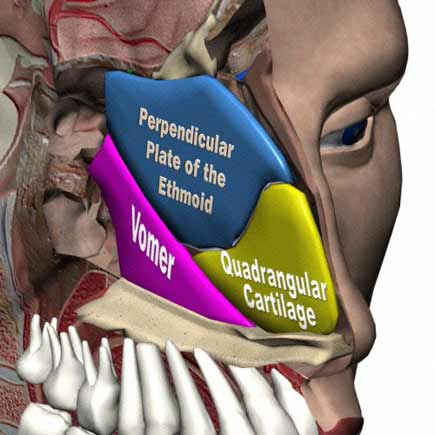
Septum:
Patient complains of recurrent nasal obstruction.
On examination the external nose is normal (there is no dorsal hump, columellar show ie.excessive show of the columella, nor retraction, no tip ptosis i.e. drooping of the tip,)
The vestibule is normal (the vestibule is examined by raising the tip of the nose with the tip of the left thumb and examined for any furuncle, crusts, vestibulitis).
Anterior rhinoscopy reveals a deviation of the cartilaginous septum, anterior or posterior deviation (with relevance to a vertical line from the nasion to the nasal spine of maxilla) with compensatory hypertrophy of the contralateral inferior turbinate (the inferior turbinate opposite to the side of the deviation will physiologically hypertrophy to minimize the airflow to prevent the excessive drying effect of increased air passage on the concave side of the deviation.)
If there is associated sinusitis, there will be mucopurelent discharge seen exuding from the middle meatus.
Cold spatula test (done with placing the flat depressing part of the tongue at room temperature underneath the nostril, and observe misting) will reveal diminished frosting of the ipsilateral side.
Cottles test (done by placing the thenar eminence of the hand in the ipsilateral nasolabial furrow and pushing outwards to open a possible collapsed nasal valve) will be negative i.e. nasal obstruction will not disappear (if it disappears, it means that the obstruction is at the level of the nasal valve and not due to the septum and what the patient requires is nasal valvular surgery.)
Postnasal examination will be normal or may show a postnasal drip if the sinuses are involved.
Next the paranasal sinuses are examined for sinus tenderness. Location: Maxillary-in the canine fossa, frontal-in the supraorbital area near the medial canthus, ethmoid-medial to the medial canthus and the sphenoid is referred to the retro-orbital or vertex region.
Diagnosis:
Patient has got a deviation of the nasal septum with compensatory hypertrophy of the inferior turbinate with or without associated sinus disease .
Investigation:
- Diagnostic nasal endoscopy to know the extent of the deviation
- Plain x-ray to know if the sinuses are involved
-Caldwell view for frontal sinuses
-Waters view for the maxillary sinus
-a combination of Caldwell and waters for the study of the
ethmoid sinuses
-Open-mouthed waters for the sphenoid sinuses
- CT: coronal ct 3mm cuts to study the paranasal sinuses if one is planning to operate on the sinuses as well.
Treatment:
If it is anterior deviation then septoplasty is the preferred mode of surgical treatment since the anterior septum is essential to maintain the integrity of the external architecture of the nose.
If its a posterior deviation, then smr can be done if the patient is more than 18 years of age. There is a growth center in the posterior half of the cartilaginous septum and if smr is done less than 18yrs of age, it will lead to developmental hypoplasia of the mid third of the face.
If the inferior turbinate is grossly hypertrophied then it can be dealt with eiither submucosal diathermy, turbinectomy or turbinoplasty.
Points:
- For all nose cases, smell should be assessed ..UPSIT (University of Pennsylvania Smell Identification Test) is the standardized method of smell assessment.
- Objective assessment of nasal obstruction is by rhinomanometry.
- Complications of surgery include septal haematoma, septal perforation.
Tonsil:
Patient complains of recurrent sore throat especially while consuming cold drinks.
(cold is a viral activator and activates harboured viruses to proliferate become virulent)
On examination:
Oral cavity:
The lips, angle of the mouth, vestibule, gingival, teeth, buccal mucosa and gingivobuccal Sulcus is normal.
The anterior two thirds of the tongue, floor of mouth, hard palate are normal
Oropharynx:
In the Oropharynx,
The anterior pillars are congested. The tonsils are hypertrophied (if it extends beyond the limit of the posterior pillar. Uvula is normal. Posterior third of tongue is normal (best seen by ILS mirror)
Postnasal exam may show adenoid hypertrophy.
Neck Examination:
Jugulodigastric nodes (woods node) may be enlarged and tender (if there is infection)
Signs of infection:
Congestion of the anterior pillars
Tender JD nodes
Implications:
Should not operate when there is an infectiont here will be severe bleeding.
Investigation:
Hb (should not operated when Hb less than 10gms %)
BT CT (to rule out bleeding tendencies)
ESR (to rule out infections high esr)
TC DC.
Urine (urine sugar..to rule out diabetes)
Treatment:
If there is active infection:
Broad-spectrum antibiotic
If there is no infection, in chronic tonsillitis
Tonsillectomy.
CSOM-tubotympanic (safe).
Patient complains of recurrent ear discharge, profuse, non foul-smelling, aggravated especially during an upper respiratory infection.
Explanation:
- Called tubotympanic disease since the infection ascends from the nasopharynx through the Eustachian tube to involve the tympanum or the middle ear therefore called tubotympanic. This follows either an upper respiratory tract infection or as a result sinus disease(acute or chronic) since the secretions from the sinus are wafted down the lateral wall of the pharynx ,almost washing the tubal orifice from here, the infection can ascend via the eustachian tube to the middle ear.
- Profuse discharge since the disease primarily involves the anterior anterior part of the middle ear which contain plenty of goblet cells which secrete profuse mucous.
- Safe, since the tympanic membrane perforation is central and is surrounded by a collar of residual membrane-this acts as a barrier preventing the inward migration of outer ear canal skin into the middle ear manifesting as Cholesteatoma.
- Non-foul smelling since there is no osteitis nor anaerobic infection.
On examination:
Inspection:
Pinna, preauricular, postauricular and external auditory canal are normal (i.e. no deformity of the pinna, pre and postauricular nodes are absent, no preauricular sinus or fistula, no otitis external, furuncle ).
The cartilaginous lateral portion of the external auditory canal should be evaluated for furuncles and sebaceous cysts. Furuncles will be tender; sebaceous cysts will be painless unless they are infected. Dry, flaking skin of the lateral external auditory canal often associated with minimal cerumen suggests chronic seborrheic dermatitis
There is a central perforation of the tympanic membrane (describe small, medium, kidney shaped, subtotal perforation involving which quadrant)
There margins of the perforation are well defined. There maybe mucopurelent discharge from the perforation. Through the perforation the mucosa of the middle ear may be visualized..the mucosa of the middle ear maybe congested polypoidal or granular.
Palpation:
There is no tenderness of the cymba concha, which overlies the MacEvans triangle, deep to which is the mastoid antrum suggesting absence of antral disease, and there is no mastoid tenderness suggesting absence of involvement of the mastoid bone.
Fistula Test:
If there is fistulatous communication of the middle ear to the inner ear , then, on compressing the tragus and increasing the pressure in the external canal, this is transmitted to the middle and through the fistula into the inner ear labyrinth causing vertigo. If there is no fistula, then the fistula test will be negative.
Facial nerve: if the facial nerve has been involved due to middle ear disease,, there will be signs of facial nerve paralysis. There integrity of the facial nerve should therefore be assessed in all middle ear disease cases.
Tuning for tests:
Severity of hearing: Rinne's Test
|
Severity |
256 hz |
512 hz |
1024 hz |
|
mild |
- ve |
+ ve |
+ve |
|
moderate |
-ve |
-ve |
+ve |
|
severe |
-ve |
-ve |
-ve |
Therefore, based on the rinne's test it is possible to assess the severity of hearing .
Webers test:
By placing a vibrating tuning fork on the forhead, the sound will be lateralised to the affected ear.
ABC test :equal
Will show that there is no sensorineural component (sensory: cochlea, neural: auditory nerve) and that there is adequate cochlear reserve to perform Tympanoplasty.
If there is sensorineural disease, middle-ear reconstructive surgery will not give adequate hearing improvement.
The hearing loss from the perforation alone will typically range form 0 to 35 dB.
Damage to the ossicles is suggested preoperatively by a conductive hearing loss of 40 dB or greater, and the tympanogram (type AD) may be confirmatory.
Diagnosis: Important
Patient has got a left (or right) sided chronic Suppurative otitis media of the tubotympanic variety in the active (or in inactive, quiescent or healed ) stage with conductive hearing loss with negative fistula sign and intact facial nerve.
Investigation:
Pus for culture and sensitivity-to know the microbiological profile.
X-ray mastoid-to know whether there is mastoid involvement, to know the position of the dura(if there is a low lying dura) to know the position of the sinus plate(if there is a forward lying sinus plate) and if there is a Korners septum-all this if one is contemplating mastoid surgery.
Audiogram -¦to know the extent of hearing impairment .if there is greater than 40 db conductive hearng loss, then there maybe Ossicular disruption and ossiculoplasty may need to be undertaken.
Treatment:
If the ear has been dry for six weeks, the perforation can be closed by myringoplasty.
This can be done either as an overlay, underlay or interlay technique.
Type 1 tympanoplasty.
If the integrity of the ossicular chain is assessed by elevating the tympanomeatal flap, putting a drop of saline on the round window area and giving a gentle tap of the malleus handle, the impulse is carried through the ossicular chain, via the scala vestibuli, helicotrema, scala tympani and manifesting as a bulge in the round window which is not visualized since the round window lies in a recessed niche and therefore inferred from the bulge of the saline drop in the round window area.
If there is an ossicular defect , then the ossicular chain can be reconstructed by a partial ossicuolar reconstruction prosthesis ie PORP or a total ossicular replacement prosthesis.
If surgery cannot be undertaken hearing can be rehabilated using a hearing aid.
Types of hearing aid:
Body worn, behind the ear, in the canal, completely in the canal.
If there is continuous discharge, then a bone anchored hearing aid (BAHA) can be given.
The most recent are digital programmable hearing aids and middle ear implantable hearing aids.
Nasal Polyp:
Definition:
A polyp is an oedematous hypertrophied protrusion of mucosa from a sinus through its ostia, containing a variable degree of round cell infiltrate,pale translusent and insensitive to touch and traversed on its surface by faint blood vessels.
On examination.
The external nose is normal .
Anterior rhinospopy reveals :
1. In a case of antrochonal polyp, a pale,glistening mass within the nasal cavity.Its insensitive to touch and can be probed all around.This is to distuinguish from an inferior turbinate which is reddish, sensitive to touch and cannot be probed all around since its attached to the lateral nasal wall.
In cold spatula test, there maybe diminished frosting on the ipsilateral side.It is of infective etiology and the polyp exits from the antrum through its accessory ostia.While it is still within the nasal cavity its called and antronasal polyp when once gains access to the choana due to its posterior growth, its called an antrochonal polyp
2.In a case ethmoid polyp,the polyps are multiple (since they arise from the multiple honey combed cells of the ethmoidal complex.) and bilateral generally.It is due to an allergic etiology.
Investigation:
Detailed cut(3mm) coronal CT
Treatment is surgical.
1.Antronasal polyp...after polypectomy, Middle meatal antrotomy is done...this generally prevents a recurrence.
2.Bilateral multiethmoidal polyp.:Intranasal endoscopic ethmoidectomy ..this is the definitive treatment and generally prevents a recurrence.Today a powered instrument to remove the polyp..this is called a microdebrider and makes the procedure quicker.